It’s been a time of great unrest in the Unites States and around the world after the death of George Floyd in Minneapolis at the hands of several police officers there. Demonstrations continue to occur around the country. Unquestionably we’ll see some disease surges in cities where protests occurred. Some factors that could lead to a greater surge include the use of tear gas and pepper spray which induce violent coughing, a significant driver of disease spread. Additionally, pepper spray and tear gas cause respiratory epithelial damage which could make protesters more susceptible. We know from sporting events like the UEFA Champion’s League match in Milan on February 19 between between Atalanta and Valencia that the gathering of thousands of screaming people can lead to devastating super-spreading events. Two days after that match Italy had its first case and epidemiologists feel that the match likely played a part in the region’s massive outbreak. Similarly, the protests saw much yelling likely introducing more virus into the air and onto surfaces. A mitigating factor of course, is that almost all protests occurred outdoors where dissipation of virus containing droplets occurs much faster than the still air inside buildings. We’ll likely start to see increasing cases in the next week as spikes generally occur 2-3 weeks after spreading events. Admittedly though, since there’s already a significant increase occurring in many localities due to reopening measures it may be hard to tease out causative factors.
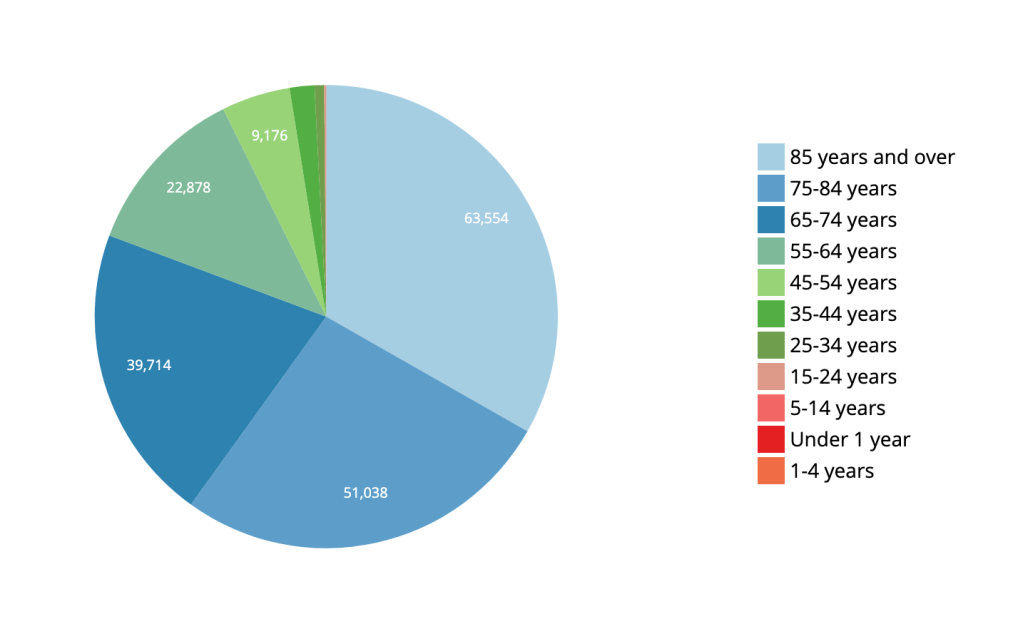
There’s a bit of a notion that COVID-19 is merely a disease of the very old. While this disease unquestionably hits older ages disproportionately, the death toll for people pre-retirement age and younger is not insignificant. In the US, 19% of all deaths have occurred in ages 64 and below for a total of 36,906 deaths at the time of this writing. COVID-19’s disease burden is not limited to retirees and the risk to older, pre-retirement workers is substantial. This has impacts beyond death rates. The disease often leads to a long period of illness and potentially long hospitalizations. Having a significant number of employed individuals hospitalized and/or sick for extended periods of time has a measurable effect on the economy. Dismissing this disease as merely a disease of the very old is not just statistically wrong, it’s unwise on many levels for the wellbeing of the nation.
CDC Data for US COVID-19 Deaths by Age/CDC
A MMRW Early Release publication looked at how the US Air Force managed over 10,000 trainees and limited total COVID-19 cases to 5 with only 3 transmissions. Their success is no surprise to public health experts as it followed well established non-pharmaceutical interventions. Trainees were kept healthy utilizing arrival quarantine, social distancing, mandatory face coverings and rapid identification of exposed/infected individuals through rapid testing and contact tracing. As the disease grew around the country, recruits from heavily infected areas were not permitted onto the base for training. The success there indicates clearly that well-established public health interventions like those described above can very successfully prevent viral spread and can allow for business almost as usual. Just because it can’t be said too much–wear a face covering!!
The FDA rescinded its Emergency Use Authorization for hydroxychloroquine today after reviewing the growing data demonstrating that the medication is ineffective in the treatment of COVID-19 and carries significant cardiac risk. There are still a few large trials underway examining the medication’s usefulness and safety but the FDA’s action means the medication now should not be used outside of those trials.
There are over 135 vaccines in development for COVID-19. The most advanced trial (Phase III) is the Oxford University vaccine which is a viral vector vaccine–the spike protein from SARS-CoV-2 is delivered with a safe virus in order to generate an immune response. In the case of the Oxford vaccine that virus is an adenovirus which causes the common cold. Early data indicates that the Oxford vaccine may not prevent SARS-CoV-2 infection but it may prevent fatal illness. Even that would make the vaccine a significant step forward against COVID-19. Right on Oxford’s heels is the Moderna vaccine which is a genetic vaccine (the mechanism was discussed in an earlier post). Moderna expects to have a large scale Phase III trial underway in July. If these vaccines make it through their trials and demonstrate efficacy and safety, it’s possible that emergency use for front-line healthcare workers, first responders and highest risk individuals may be possible in late 2020. So much has to line up for that to be a reality I hesitate to mention it for fear of raising hopes too much. But it’s always nice to end on an optimistic note so here’s to hope!
Governor Newsom relaxed California’s requirements for accelerated reopening. The new criteria focus less on how many deaths a county or municipality have and more on the number of cases. The new criteria will allow for up to 25 cases per 100,000 members of the population and no more than an 8% positive test rate. This was a major sticking point for larger counties as the previous criteria required a county have no deaths before they could reopen. It’s estimated that 53 out of 58 counties could be eligible to accelerate their reopening under these new requirements.
Drug maker Moderna announced yesterday that its COVID-19 vaccine passed an important test. This early phase included 8 people and results have demonstrated that the vaccine was safe for them and that it produced a strong anti-COVID-19 antibody response. The company then studied those antibodies in the lab and found that they had a neutralizing effect on SARS-CoV-2 in vitro (scientific term for in a testtube). This is a standard approach and generally bodes well for an antibody’s ability to neutralize the virus in vivo (scientific term for in a living organism). Moderna’s approach to vaccines is different. Traditionally a vaccine contains inactivated virus or virus proteins which when injected into the body fool the immune system into thinking a real virus is present. The body then starts making antibodies to the harmless version of the virus. Once antibodies are present, they can mount an effective immune response when exposed to the real thing. Moderna instead uses something called an RNA vaccine. Instead of injecting virus bits or inactivated virus, they inject actual mRNA (genetic material) which codes for specific proteins on or in the virus itself (e.g. spike protein important for viral entry into a human cell). If Moderna had injected DNA into the the body there might be a risk of that DNA disrupting the body’s normal genetic code, but mRNA doesn’t incorporate into our genes, it only gets read to make protein. Once the vaccine mRNA is in the body actually starts creating the protein from the pathogen and expressing it on cell surfaces which is then recognized by memory cells allowing an immune response to a virus that the body has never actually seen. When a real virus invades, the body is ready for it and attacks it before it can do real damage. This type of vaccine has some advantages over traditional vaccines. They can be produced more quickly and more cheaply, they are less dangerous for patients since there’s no virus being used for the immune response and they can be scaled up quickly for mass vaccinations during a pandemic. Moderna plans to move on to their next phase of testing which will be an expansion to around 600 patients. Very good news indeed, but remember it’s still a long way to knowing for sure that this vaccine works and is safe.
More and more data is showing that we could very effectively control the virus if we quarantined our mouth and nose more effectively. If 80% of the population was fully compliant with wearing masks whenever in public, the data shows we could stop the spread of this virus. This, of course, could have major implications for reopening our society and getting businesses back up and running. For an excellent dive into the importance of masks take a look at this must-read.
For some time I’ve been considering leaving Facebook. While there are many positive aspects of the social media giant, there are some things about it that I find hard to stomach. It’s a great place to share photos of family and pets and jiu jitsu, but it’s a terrible place for conversations. The world is polarized and so is Facebook, actually, the world may be polarized because of Facebook. I love to talk science though. Writing about COVID-19, while not a cheery subject, has helped me process some of the feelings I have about living through it, especially as a public health physician, worried father and husband. I just want to do it more on my terms. No yelling, no anti-science comments, just people who want to understand what on earth is happening right now with the best tool the human race has ever devised for understanding our world. So welcome to my new home!
Thoughts on COVID-19
Nationally there’s a bit of a worrisome trend with our doubling time. A while back, on Facebook, I mentioned the good news that our national doubling time was increasing and that it was increasing by more than a day, every day. That signifies a peak in terms of new daily cases. The daily increase in doubling time was actually increasing along a sloping curve meaning something approximating an accelerating growth curve. That’s not happening anymore. What we see now is more of a plateauing of our doubling time. It’s been stuck increasing at a rate of about 18-20 hours a day for a week or so–every day our doubling time is increasing by the same amount, 18-20 hours. It’s no longer accelerating. There are a couple reasons for why that might be happening. Some are okay, some are not. It’s possible that regional and state differences in the timing and slope of the COVID-19 curves are making it so that later peaking states are rising while earlier peaking states are waning. That could be okay. It just means we’re all marching to the beat of our own drums and eventually we’ll all start a collective increase in our doubling time rate together. It also could mean that people are slipping with their social distancing and stay-at-home compliance. Spread of infection during recent protests along with religious ceremonies for Easter and Passover could be putting the brakes on our ride away from the peak. More time will tell. For all sorts of great information on the national doubling time, visit https://www.danreichart.com/covid19 He runs one of my favorite statistical sites for COVID-19 and most of my US doubling time information posted to Facebook and now here comes from his great work. His approach is to look at each day anew. Here’s where we are today and this is what we’ll look like in the future if our doubling time stays what it is today.
And now some pretty good news. Scientists from the the Jenner Institute at Oxford have been working on a vaccine. What makes this good news is that it’s a vaccine they made some time ago as a possible vaccine for MERS and they’ve already tested it for safety–last year actually. Safety testing can be one of the longest steps in the process of making a good vaccine. You have to watch people for quite a while to make sure they don’t have any lingering adverse effects–sometimes several years. Having something ready to test for efficacy is a big head-start. The vaccine has recently been tested in rhesus macaque monkeys with good results. Six monkeys were given the vaccine and then exposed to a large amount of the virus. All six are still healthy a month out. Testing in monkeys doesn’t guarantee success in humans but the rhesus macaque is just about the closest thing we have to humans. Given that, testing in humans is likely to happen sooner rather than later. If all goes well (that’s a gigantic IF), and the Institute is given emergency approval, they could have several million doses available as early as September. That would be monumental. Please remember there are still massive efficacy hurdles to jump so take a deep breath and in a very unscientific way, maybe cross your fingers.
With this pandemic, the rush to find an effective treatment has been fully understandable. I posted early about the possibility that hydroxychloroquine might be an effective treatment based on some very small, and it turns out pretty flawed, studies. Newer (also small, also not peer reviewed) studies out of Brazil and the VA system in the US indicate that hydroxychloroquine is ineffective in the treatment of COVID-19 and possibly dangerous (the trial in Brazil was stopped when some of the patients in the high-dose arm of the study developed lethal cardiac arrhythmias). The efficacy and safety of hydroxychloroquine to treat COVID-19 should be established in large, controlled studies and it should not be provided as an off-label treatment for the virus in a non-study setting. There, I said it. Good science takes time and patience. But nobody’s listening to me.
Look to hear from California’s Governor Newsom sometime in the next 48 hours regarding details about relaxation of the stay-at-home/social distancing orders. California’s actions have made a difference. As we’ve known for a century at least, social distancing works and it worked here. While the initial orders were emergent and broad-sweeping, look for the relaxation orders to be more surgical and to come with a period of evaluation. We needed quick, blanket action to prevent massive spread of the virus through the entire population of California when it was doubling every two days. With a doubling time of two days, the virus would have hit everyone in America within about 40 days. Now that we’re much more under control we can relax elements of social distancing one at a time with a period of observation to look for spikes. We can then see which of these measures were the most important in preventing spread of this virus. This process will give us valuable data and will help us in the fall when it’s likely the virus will surge again. Our break from the lockdown may not be as soon as we’d hoped though. This past weekend, some Californians jumped the gun and flocked to the beaches in numbers that are simply unwise at this point. This was a mistake and may very well lead to an uptick in the virus within the next two weeks. It’s just simple virology. If that happens we may not get our relaxation phase as soon as we would have, had people maintained social distancing per state and local public health department orders. Here’s hoping we don’t see that or that what we see isn’t enough to derail our break from the lockdown.