It’s been a time of great unrest in the Unites States and around the world after the death of George Floyd in Minneapolis at the hands of several police officers there. Demonstrations continue to occur around the country. Unquestionably we’ll see some disease surges in cities where protests occurred. Some factors that could lead to a greater surge include the use of tear gas and pepper spray which induce violent coughing, a significant driver of disease spread. Additionally, pepper spray and tear gas cause respiratory epithelial damage which could make protesters more susceptible. We know from sporting events like the UEFA Champion’s League match in Milan on February 19 between between Atalanta and Valencia that the gathering of thousands of screaming people can lead to devastating super-spreading events. Two days after that match Italy had its first case and epidemiologists feel that the match likely played a part in the region’s massive outbreak. Similarly, the protests saw much yelling likely introducing more virus into the air and onto surfaces. A mitigating factor of course, is that almost all protests occurred outdoors where dissipation of virus containing droplets occurs much faster than the still air inside buildings. We’ll likely start to see increasing cases in the next week as spikes generally occur 2-3 weeks after spreading events. Admittedly though, since there’s already a significant increase occurring in many localities due to reopening measures it may be hard to tease out causative factors.
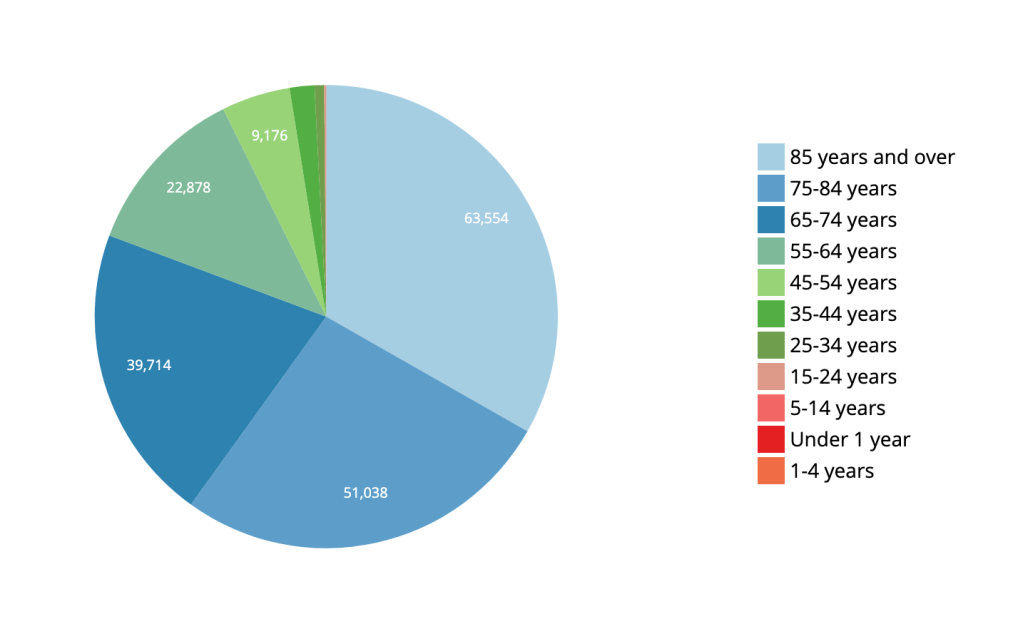
There’s a bit of a notion that COVID-19 is merely a disease of the very old. While this disease unquestionably hits older ages disproportionately, the death toll for people pre-retirement age and younger is not insignificant. In the US, 19% of all deaths have occurred in ages 64 and below for a total of 36,906 deaths at the time of this writing. COVID-19’s disease burden is not limited to retirees and the risk to older, pre-retirement workers is substantial. This has impacts beyond death rates. The disease often leads to a long period of illness and potentially long hospitalizations. Having a significant number of employed individuals hospitalized and/or sick for extended periods of time has a measurable effect on the economy. Dismissing this disease as merely a disease of the very old is not just statistically wrong, it’s unwise on many levels for the wellbeing of the nation.
CDC Data for US COVID-19 Deaths by Age/CDC
A MMRW Early Release publication looked at how the US Air Force managed over 10,000 trainees and limited total COVID-19 cases to 5 with only 3 transmissions. Their success is no surprise to public health experts as it followed well established non-pharmaceutical interventions. Trainees were kept healthy utilizing arrival quarantine, social distancing, mandatory face coverings and rapid identification of exposed/infected individuals through rapid testing and contact tracing. As the disease grew around the country, recruits from heavily infected areas were not permitted onto the base for training. The success there indicates clearly that well-established public health interventions like those described above can very successfully prevent viral spread and can allow for business almost as usual. Just because it can’t be said too much–wear a face covering!!
The FDA rescinded its Emergency Use Authorization for hydroxychloroquine today after reviewing the growing data demonstrating that the medication is ineffective in the treatment of COVID-19 and carries significant cardiac risk. There are still a few large trials underway examining the medication’s usefulness and safety but the FDA’s action means the medication now should not be used outside of those trials.
There are over 135 vaccines in development for COVID-19. The most advanced trial (Phase III) is the Oxford University vaccine which is a viral vector vaccine–the spike protein from SARS-CoV-2 is delivered with a safe virus in order to generate an immune response. In the case of the Oxford vaccine that virus is an adenovirus which causes the common cold. Early data indicates that the Oxford vaccine may not prevent SARS-CoV-2 infection but it may prevent fatal illness. Even that would make the vaccine a significant step forward against COVID-19. Right on Oxford’s heels is the Moderna vaccine which is a genetic vaccine (the mechanism was discussed in an earlier post). Moderna expects to have a large scale Phase III trial underway in July. If these vaccines make it through their trials and demonstrate efficacy and safety, it’s possible that emergency use for front-line healthcare workers, first responders and highest risk individuals may be possible in late 2020. So much has to line up for that to be a reality I hesitate to mention it for fear of raising hopes too much. But it’s always nice to end on an optimistic note so here’s to hope!
Mother and child during COVID-19 crisis/https://www.vperemen.com/Wikimedia Commons
Last week I was on call for public health and wasn’t able to post much. This long weekendwas about recovering from call. Hopefully I’ll get back into a more regular schedule this week.
The Basic Reproduction Number (R0/R-naught) for the US looks like it has crossed back above 1 for the whole country. The R0 is important if you remember because it describes how many people on average are infected by one person. As long as that number is below 1, COVID-19 cases will drop. Once it goes above one as it has now (estimated by Youyang Gu on his site) we’ll start to see overall increases in new cases of the virus nationwide.
Imperial College’s new study (not yet peer reviewed) reveals that 24 states have COVID-19 reproduction numbers that are above 1 (one) and therefore have growth of the virus. Their model which incorporates changing mobility of the population further reveals that only 15.7% of US states have truly credible reproduction numbers below 1 (one).
An article in Pediatrics examined the role children play in spreading COVID-19. Swiss researchers looked at family clusters of infected individuals and found that child to adult spread occurred in only 8% of cases. It was far more common for adults to spread the virus to their children. If this is true and validated by other studies it could have significant implications for the reopening of schools. It’s important to remember that children may still be important vectors for the disease since they have have a higher likelihood of having few or no symptoms even if they don’t spread the virus as commonly as adults do.
There were 675 new cases of COVID-19 in Riverside County over the Memorial Day weekend from Friday to Tuesday. This is a significant bump with an average of 168 cases per day over the four days. A few weeks ago, the county had been averaging under 100 cases per day. This increase is worrisome and very likely due to several factors including spread during Mother’s Day gatherings 2 weeks ago. Citizens of Riverside County have been much more mobile in recent weeks and now have a failing grade with Unacast Social Distancing Scorecard. It’s also likely that social distancing is less rigorous in general as quarantine fatigue has fully set in. Additionally, face coverings are no longer mandatory in Riverside county, an order rescinded by the Board of Supervisors–this factor alone may play the largest role in increasing numbers now and in future weeks. One might suggest that increased testing is responsible for the bump but testing is actually down in Riverside County so in all likelihood, we’re seeing higher numbers because the virus is spreading more. This is what viruses do when given the chance. As the county opens up under the Governor’s new criteria and people feel more comfortable congregating in churches, at the beach, in restaurants and in stores, look for the daily new cases to climb further.
The Washington Post is reporting that cell phone data tracked by the University of Maryland’s Transportation Institute showed that tens of thousands of people flocked to Georgia after businesses were permitted to open. Over 60,000 more trips into the state were recorded than the week before the opening on April 24. Most of these travelers came from Alabama, South Carolina, Tennessee and Florida. I’ll be keeping an eye on new case data for these five states over the next 2-4 weeks to see if numbers there start to move and will post updates.
This week my home province of New Brunswick, Canada had its first new cases of COVID-19 in two weeks. At least one of the cases is travel related. The positive individuals are in the Saint John and Fredericton areas and come just as the province has begun a phased reopening. By all estimation the province’s public health department has done a superb job managing the pandemic within its borders. The new cases serve as a reminder that the virus isn’t gone and that even in communities who have done almost everything right, it will invariably find its way back in via the path of least resistance.
Though known for a while, there are increasing reports that patients with COVID-19 are suffering from abnormal blood clotting. A study published in the Annals of Internal Medicine found that 58% of 12 post-mortem examinations found deep vein thromboses in patients with COVID-19. There is a growing use of blood thinners to treat the sickest patients in centers around the country. It’s difficult to know at this point whether these clots are part of a well known medical phenomenon related to severe inflammatory states and shock called disseminated intravascular coagulation (DIC). In DIC, extremely ill patients both bleed too much and clot too much at the same time–it’s a clotting system gone haywire and a very difficult problem to manage in critically ill patients. Some of my worst nights during training were spent at a kid’s bedside trying to get them to stop bleeding and clotting, a tragically difficult task. It could also be that there’s something about COVID-19 that specifically causes abnormal clots to develop. Large scale studies are needed to determine the cause and to sort out appropriate treatment but blood thinners seem to be working their way into current standards of care.
Coronary Artery Aneurism in Kawasaki Disease/Wikimedia
Doctors in New York have issued an advisory warning of a possible inflammatory complication of COVID-19 in children. Sixty-four kids in New York have developed a condition described as an inflammatory syndrome affecting multiple systems including the heart and blood vessels. The syndrome appears to be similar to another more well-known pediatric condition called Kawasaki Disease. Children with Kawasaki Disease have prolonged fever, rash, enlarged lymph nodes, red lips and tongue, joint pains, swollen hands and feet, and conjunctivitis without discharge or pus. Kids with Kawasaki Disease are at risk for inflammatory changes to the coronary arteries that can cause the heart vessels to develop life-threatening aneurisms. While the new COVID-19 related syndrome affects the heart it’s unclear if it causes the same aneurisms as Kawasaki Disease or instead causes general inflammation of the organ. Some children with the COVID-19 related inflammatory syndrome have develop cardiovascular collapse similar in appearance to Toxic Shock Syndrome, a finding not typically seen in Kawasaki Disease.
Governor Newsom announced the start of Phase II of California’s COVID-19 response today by allowing limited pick-up service openings for businesses like book stores, sporting goods stores, and florists as early as this coming Friday. This is a measured loosening of restrictions to be sure as there’s no real congregating allowed and this is probably the most that could safely be undertaken at this point. We have not met several of the criteria outlined by infectious disease experts for safe relaxation of stay-at-home orders. In particular, while testing is increasing, we are not at the level where comprehensive evaluation of any symptomatic person can be achieved with results on the same day or within hours. Additionally, it’s not clear that daily new cases are declining let alone for 14 days straight, another of the primary relaxation criteria. Given this, it’s a bit of a risk to begin loosening of restrictions at this point but I’m guessing he hopes allowing these relatively safe activities will help put an end to the incredibly risky behavior of protesters around the state in recent days. Some experts like Dr. Robert Kim-Farley from UCLA are predicting that Phase III which will include the opening of higher risk businesses like movie theaters and gyms might occur sometime in the late summer, possibly August or September. Timelines like this are notoriously difficult to predict however, since they sometimes depend on non-medical decision making by political leaders. I wouldn’t be shocked to see that timeline bumped up somewhat.
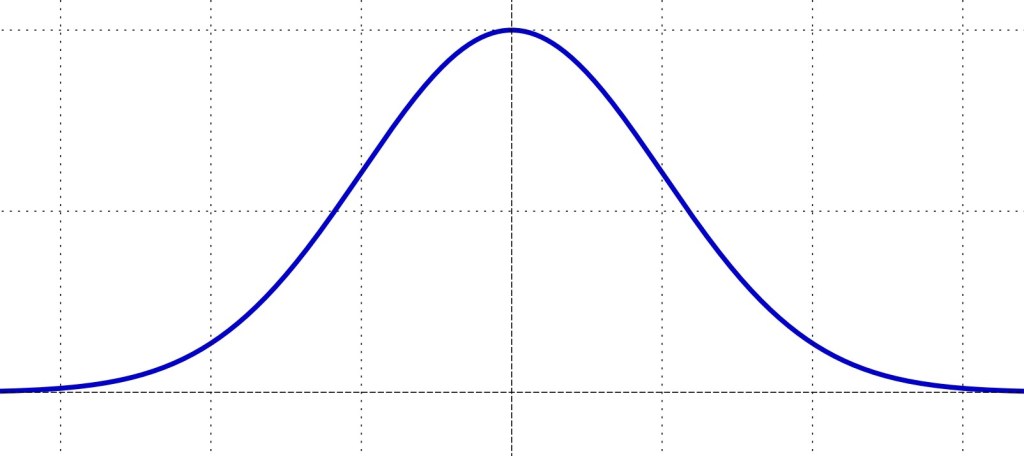
It seems pretty clear now that the United States’ COVID-19 disease course is not following a Gaussian curve with an equal slope on the way up to and down from the peak. Instead the disease is declining at a much slower rate than when it ramped up to the peak. This slow tapering recovery will unfortunately lead to significantly more cases and deaths from the initial disease surge than predicted by models that assume a Gaussian distribution as there will ultimately be more area under the curve.
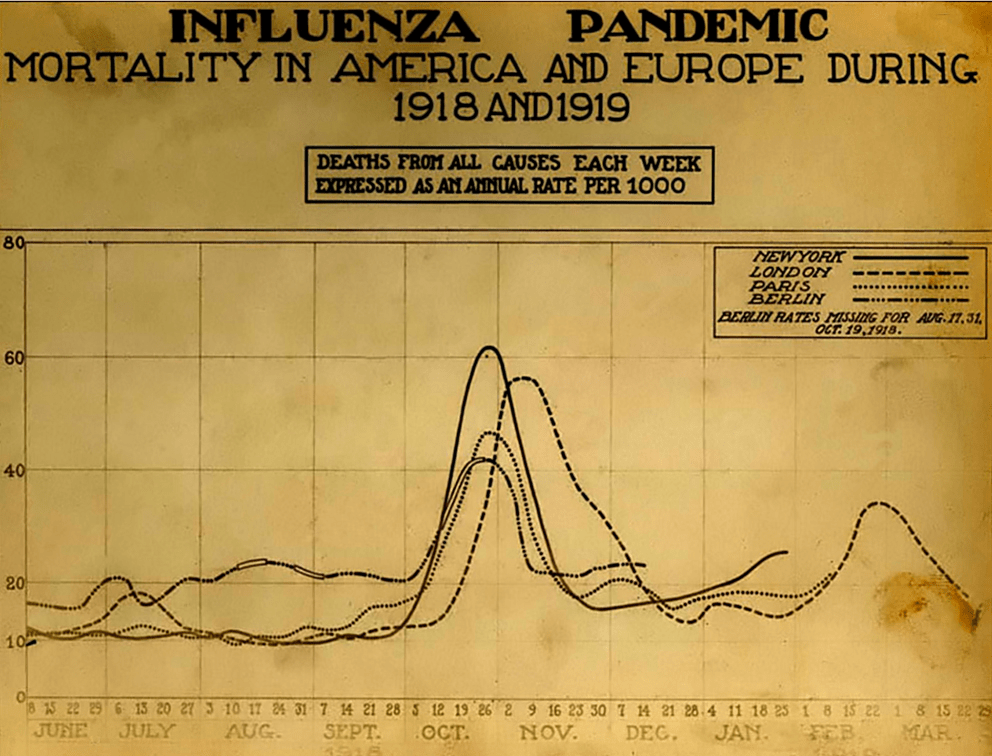
Michael Osterholm, a foremost expert on viruses and pandemics who many people saw for the first time on Joe Rogan’s podcast is the Director of the Center for Infectious Disease Research and Policy (CIDRAP). Last week his group at CIDRAP released a report that describes three possible pandemic wave scenarios based on lessons learned from previous pandemics. The first scenario sees one to two years of recurring peaks and valleys similar to what we’ve just experienced requiring periodic reinstitution of mitigation measures like we’re currently living under. For obvious reasons, this scenario could have dramatic economic repercussions. The second scenario mimics the 1918 influenza pandemic which saw an initial peak in the spring and a massive, much more devastating peak in the fall after relaxation of social distancing measures during the summer. This second peak would almost certainly overwhelm our healthcare system and lead to very large numbers of deaths but would not be followed by significant peaks after the fall peak as the virus would have burned through most of the population. The third scenario describes a slow burn after the current, initial surge. In this scenario there are no peaks and valleys, just a constant relatively stable number of ongoing cases and deaths. This scenario would not require large-scale mitigation measures after the initial peak. While this pattern has not been seen with previous influenza pandemics it could occur with a novel coronavirus such as SARS-CoV-2/COVID-19. Whatever scenario plays out, the CIDRAP group advises that Americans should get used to the idea of significant COVID-19 activity for the next 18-24 months. As the pandemic starts to fade away, it’s likely that SARS-CoV-2 will continue to cause less and less severe illness over the next decade eventually settling in as a non-life threatening upper respiratory infection much like it’s other cold-causing coronavirus cousins.
Diners in Stockholm during the COVID-19 pandemic. Jonathan Nackstrand/AFP via Getty Images
Sweden’s approach to COVID-19 is different from most countries. Is it working there? Should the US have adopted this strategy? A closer look at the Swedish experience reveals significant problems with the Scandinavian country’s approach andhighlights inherent differences between the two countries that largely prohibit its application in the US.
Facing a novel Coronavirus with a doubling time of around 2 days, most of the world reacted to SARS-CoV-2 with what can only be described as justifiably draconian measures to slow the spread. Absent mitigation and with a doubling time of 2 days, the US would have seen the virus hit every American within about 40 days. America, like most of the world, enacted emergent stay-at-home and social distancing orders and closed non-essential businesses to flatten the curve. Too many infections too quickly would have completely overwhelmed the healthcare system, tragically demonstrated in Wuhan and Lombardy where the virus had a devastating head-start.
Several prominent European countries undertook a different strategy. England, the Netherlands and Sweden instituted what is considered a herd-immunity approach. While it’s important to note that England and the Netherlands had to abandon this blueprint when cases and deaths started climbing, Sweden has largely stuck with the plan. The idea behind this is that in the absence of a vaccine, the only way to move on from a virus like this is to allow herd-immunity to develop. The purest form of this approach would be to just let the virus burn through a population and allow everyone to become infected, but at the cost of thousands of lives and an overwhelmed healthcare system. Sweden didn’t go that far but instead attempted to find a middle-ground. They executed a much less restrictive approach than other nations and allowed businesses, restaurants, bars, and gyms to to stay open while enacting certain social distancing rules for the owners and patrons to follow. The Swedish government, instead of stay-at-home orders, recommended that Swedes voluntarily enact social distancing by working from home and keeping an arm’s length distance when around others. It’s somewhat like a controlled burn approach with the goal of keeping the virus down to about 30% of its normal spread while focusing on the protection of vulnerable populations.
On the surface, Sweden’s approach seems to be working for them. Without enacting strict, often unpopular laws, Sweden has effectively flattened the curve and prevented a hospital crisis. The government believes that in Stockholm at least, a significant portion of the population has been infected and that they may be closing in on herd immunity but this is a projection without solid data confirmation as comprehensive serology testing has not yet been fully undertaken. Results in Sweden have led some here in the United States to suggest that Sweden is evidence that the response to COVID-19 has been an overreaction to a virus that is not as severe as experts would have us think and that Sweden’s strategy should have been adopted here to soften the economic blow.
Let’s take a look at the Swedish experience to see whether these claims have merit and whether they could have been successfully adopted in the US.
First I think it’s important to determine whether their approach is as different as it seems. While there’s no stay-at-home order in Sweden, there are public health orders in place to increase social distancing. High schools and colleges were closed, gatherings of over 50 people are prohibited, in restaurants and bars, patrons must maintain arm’s length distance from one another. Instead of orders, Sweden called on its citizens to voluntarily enact social distancing principles. The population was asked to work from home, avoid unnecessary travel and maintain distance from others. Swedes seem to have largely adopted these measures. Data suggests that movement in the streets of Stockholm was down to 30 percent of normal, a number that in many cases surpasses US reductions in movement even in the regions most compliant with mandated stay-at-home orders. Upwards of 50% of Swedes transitioned to working from home and use of public transit dropped in half as well. Even vacations have been canceled with 85% of Swedes reporting that they would not be taking the usual annual pilgrimage to the resort island of Gotland.
Whether mandated or not, a voluntary stay-at-home policy is still a stay-at-home measure. Swedish ideology is rooted in a deep respect for social justice. Heba Habib at the Christian Science Monitor who has followed the Swedish experience with COVID-19 reports that Swedes take great pride in their personal responsibility. The idea of breaking the social contract of social distancing by holding a mass gathering or flocking to the beach at the first sign of sun would be flatly rejected by Swedes.
Sweden promotes itself as being a model society based on values of social justice and human rationality, with a high level of trust between people and trustworthy authorities. This has its origins from the Social Democrat-introduced concept of “Folkhemmet,” or people’s home, where a welfare state cares for all with the proviso that everyone complies with a communal order.
Heba Habib/Christian Science Monitor
In effect, Swedes largely trust their authorities to do what’s best for the people with respect to COVID-19 and in return they have generally complied with voluntary COVID-19 orders when asked to do so by their government. The Swedish experience with COVID-19 has been reliant on this trust in government and the importance of maintaining the social contract. Though falling somewhat in recent years, the OECD index on government trust shows Swedes trust their government quite a bit more than Americans do. For the Swedish approach to work in the US, Americans would have to show the same willingness to take the governments assessment of virus severity and subsequent social-distancing recommendations as truth and follow them without legal mandate to do so. Americans suggesting that Sweden’s approach should be ours, must honestly answer if it is part of US national identity to trust and comply with government in this way.
Trust in government: Sweden–56%, US–35%/OECD
So has the Swedish approach worked? If the only metric by which you measure success is flattening the curve to prevent overwhelming hospitals, then yes, Sweden has succeeded for now. It’s possible that Stockholm has peaked though data is not yet conclusive and it is too early to tell if the nation has peaked. Youyang Gu’s universally praised, highly predictive model estimates an overall infection rate of about 5% in Sweden; that is nowhere near numbers needed for herd immunity. It would seem there are still a lot of people left for the virus to burn through.
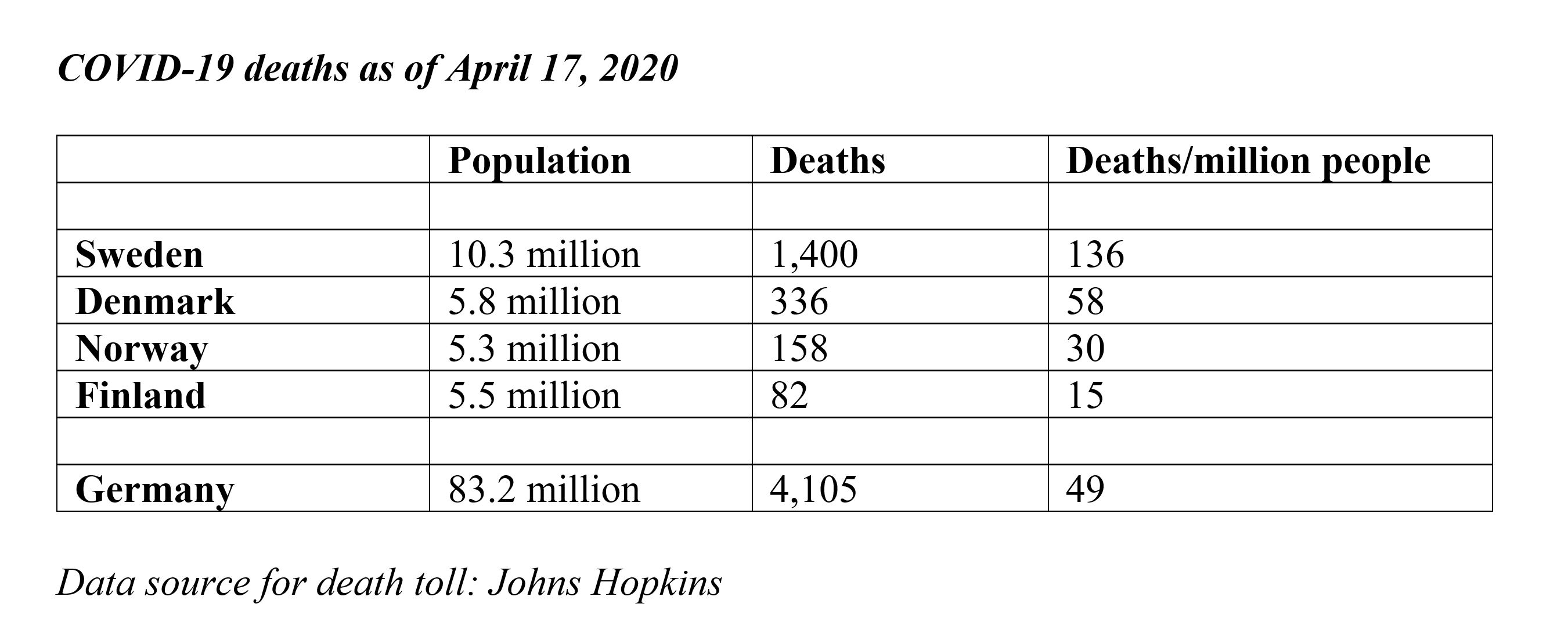
What about their deaths? Have they protected the people from dying, particularly the vulnerable? If this is the metric of success, then Sweden’s approach has not been particularly successful. Deaths in Sweden are proportionately higher than their Scandinavian neighbors who enacted stricter social distancing measures.
Total deaths and Deaths/Million People/John’s Hopkins
These deaths have hit vulnerable populations in Sweden hard. About 50% of all deaths in Sweden have occurred in elder care facilities. One of the goals of the Swedish approach was to protect these vulnerable populations; in that they have not been particularly successful. If your metric for measuring success is preventing death, particularly among the vulnerable, then Sweden has come up short.
One of the arguments made here in American by people opposed to the social distancing orders is the effect these measures have on the economy. They point to Sweden as an example of a country that has been able to keep its economy open in spite of COVID-19. If we take a closer look at their economy, however, Sweden is not fully escaping the toll this virus has taken on other nations with more aggressive lockdowns. The Swedish Finance Minister projected that the economy would shrink by 7% which was a worsening of previous projections. This contraction is similar to the projected contraction in the Netherlands and depending on how the virus behaves, could be as much as 10%. Unemployment is expected to reach 11%. That’s certainly better than the US’s expected 20-30% unemployment. It’s important to remember, however, that the Swedish government helps to prevent unemployment by giving employers money to keep people on payroll. To compensate for reduced employee hours and business productivity losses, employers are permitted to cut salaries but the government then supplements employee pay up to 90% of original salary. The US has attempted to pass legislation that similarly protects jobs by providing forgivable loans to businesses who keep people on the payroll. The roll-out has been fraught with problems and the money quickly dried up before most could benefit. Businesses have had to let people go while waiting for assistance, driving up unemployment rates. The US focus has been to provide one-time payments to most Americans and to bolster the unemployment benefits system. Sweden’s very different approach is of course paid for in part through a very different taxation strategy than in the US. The top statutory personal income tax rate in Sweden in 2018 was 57% and applies to all earners who are making 1.5 times the national average and in the US, the top rate of 43.7% applies only to people who make over 9 times the national average. I bring this up not to advocate for a Swedish welfare state or for the US to adopt the Swedish system of taxation. It is, however, important to consider the apples to oranges differences in Swedish and US economic strategies when suggesting that adopting the Swedish approach to COVID-19 would work in America or that we would see the same economic benefits.
There are other factors which make the Swedish experience somewhat unique and difficult to apply elswhere. Their population density is significantly lower and they have far less travel into the country than their harder hit neighbors in Europe. Inbound tourism is dwarfed by countries like Spain, Italy and France and the US. According to the World Tourism Organization, in 2017, Sweden had 7M inbound tourists compared with almost 77M inbound tourist to the US. With fewer people traveling into the country, Sweden was able to avoid massive importation of the virus making their initial contact tracing efforts exponentially easier to manage.
So this has all been a long-winded way of saying that Sweden’s approach is not the panacea some in the United States claim. In fact, 22 of Sweden’s top research and infectious disease scientists recently wrote an op-ed in a national newspaper calling on the government to enact strict social-distancing and stay-at-home orders matching other nations. They’re concerned about Sweden’s high number of deaths and continuing increases in new daily cases, especially in vulnerable populations. As they see it, Sweden is headed for a disastrous surge in cases which could soon overwhelm their healthcare system.
I can’t say that Sweden has been completely wrong-headed about their approach. It’s simply too early to tell. The world should study their model and learn from it to see if it ultimately demonstrates a benefit. A comprehensive review of all the factors that contribute to a nation’s success or failure in the fight against COVID-19 is far beyond the scope of this blog post and, frankly, beyond the knowledge of its author. My goal here is to simply point out that fundamental differences in our two countries make for difficult comparisons and tougher still, conclusions. The idea that the Swedish experience proves the public health response in the US was an overreaction to an overhyped virus is unsupported by the facts. It’s also folly to suggest that the Swedish model, not yet shown to be successful even in Sweden, would work in America. The differences between our two countries both physically and temperamentally are vast. Ignoring these fundamental differences and assuming that the Swedish approach to COVID-19 would be successful if adopted here is woefully naive even if politically expedient.
Time will tell if the Swedes have successfully ridden the wave of COVID-19 into herd immunity without the need for government orders, or if all they’ve done is push their peak down the road a bit and that dark days lie ahead for them.
This is a common and somewhat understandable refrain in recent months. Is the damage to the economy caused by public health interventions like social distancing and shelter-in-place worse than the potential damage of COVID-19 itself? Is the cure worse than the disease? How can we know?
“The farther backward you can look, the farther forward you are likely to see.”
Winston Churchill
History can help us if we’re willing to learn from it. Several economists have taken a bite out of this problem with very interesting results. Prof. Emil Verner from the MIT Sloan School of Management along with Dr. Sergio Correia and Dr. Stephan Luck from the Federal Reserve have done what more of us should do–learn from history. Together these economists studied social distancing practices or non-pharmaceutical interventions (NPIs) from the Spanish Flu of 1918 to evaluate the effects of social distancing on the economy. Their paper is not yet peer-reviewed but it provides some compelling insights into the efficacy of public health interventions in a pandemic and the resulting economic impacts.
The 1918 influenza pandemic is thought to have infected nearly a third of the world’s population at the time or 500 million people. In the United States alone, 675,000 people died, worldwide–50 million. It was caused by an H1N1 virus with genes of avian origin. Public health measures at the time were focused on prevention of spread from person to person. Those infected were prevented from breathing the same air as the uninfected. Public health guidelines and interventions at the time included prohibiting mass gatherings, banning non-essential meetings, closing dance halls, bars and cinemas, and some encouraged staggered work times to prevent unnecessary congregation. All pretty familiar stuff today, right? Like today, the degree to which these recommendations were followed varied widely throughout the country.
Policemen in Seattle wearing masks during the 1918 Influenza pandemic/National Archives
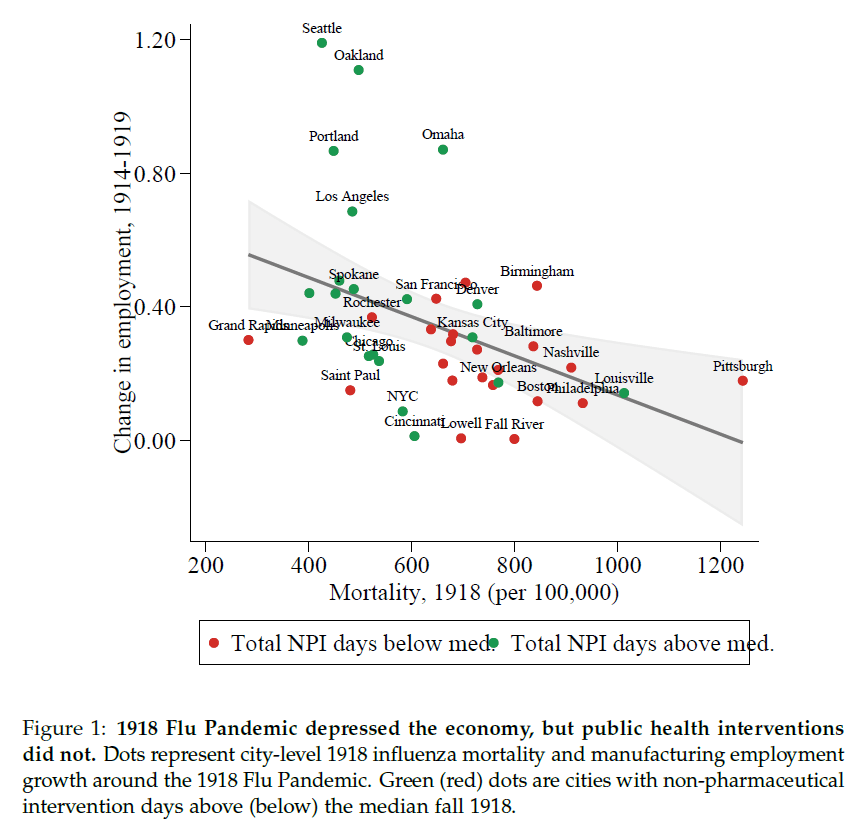
What Verner, Correia and Luck found was that, as expected, higher mortality in a region led to greater economic depression. More than that though, they looked at American Cities’ response and compared the economic impact of municipalities who enacted strict social distancing measures with those who enacted much weaker measures. Here they found that cities who enacted the strictest social distancing measures had lower mortality but they also experienced the greatest economic growth. Simply put, cities that were committed to public health measures like social distancing had fewer deaths and better economic outcomes.
The green-dot cities in the upper left who enacted strict NPIs like social distancing over longer periods had lower mortality and higher economic growth whereas the red-dot cities in the lower right, who were more lenient with NPIs, experienced higher mortality and stunted economic growth. The authors say it best.
Comparing cities by the speed and aggressiveness of NPIs, we find that early and forceful NPIs do not worsen the economic downturn. On the contrary, cities that intervened earlier and more aggressively experience a relative increase in manufacturing employment, manufacturing output, and bank assets in 1919, after the end of the pandemic.
Emil Verner, Dr. Sergio Correia and Dr. Stephan Luck/Pandemics Depress the Economy, Public Health Interventions Do Not: Evidence from the 1918 Flu
The economic impacts of this pandemic on families and businesses has been devastating. Public health measures like shelter-in-place and social distancing are a bitter pill to be sure. History tells us, however, that this medicine, while hard to swallow, gives us the best chance of surviving, both medically and economically.
Future generations will study this moment, perhaps as they face their own crisis. Just like us they’ll be looking for clues from the past about how to survive. Will they see ancestors rooted in solid science with an unwavering commitment to public health, or will they see a fleeing from science and reason when things got hard? I’m not sure.
For some time I’ve been considering leaving Facebook. While there are many positive aspects of the social media giant, there are some things about it that I find hard to stomach. It’s a great place to share photos of family and pets and jiu jitsu, but it’s a terrible place for conversations. The world is polarized and so is Facebook, actually, the world may be polarized because of Facebook. I love to talk science though. Writing about COVID-19, while not a cheery subject, has helped me process some of the feelings I have about living through it, especially as a public health physician, worried father and husband. I just want to do it more on my terms. No yelling, no anti-science comments, just people who want to understand what on earth is happening right now with the best tool the human race has ever devised for understanding our world. So welcome to my new home!
Thoughts on COVID-19
Nationally there’s a bit of a worrisome trend with our doubling time. A while back, on Facebook, I mentioned the good news that our national doubling time was increasing and that it was increasing by more than a day, every day. That signifies a peak in terms of new daily cases. The daily increase in doubling time was actually increasing along a sloping curve meaning something approximating an accelerating growth curve. That’s not happening anymore. What we see now is more of a plateauing of our doubling time. It’s been stuck increasing at a rate of about 18-20 hours a day for a week or so–every day our doubling time is increasing by the same amount, 18-20 hours. It’s no longer accelerating. There are a couple reasons for why that might be happening. Some are okay, some are not. It’s possible that regional and state differences in the timing and slope of the COVID-19 curves are making it so that later peaking states are rising while earlier peaking states are waning. That could be okay. It just means we’re all marching to the beat of our own drums and eventually we’ll all start a collective increase in our doubling time rate together. It also could mean that people are slipping with their social distancing and stay-at-home compliance. Spread of infection during recent protests along with religious ceremonies for Easter and Passover could be putting the brakes on our ride away from the peak. More time will tell. For all sorts of great information on the national doubling time, visit https://www.danreichart.com/covid19 He runs one of my favorite statistical sites for COVID-19 and most of my US doubling time information posted to Facebook and now here comes from his great work. His approach is to look at each day anew. Here’s where we are today and this is what we’ll look like in the future if our doubling time stays what it is today.
And now some pretty good news. Scientists from the the Jenner Institute at Oxford have been working on a vaccine. What makes this good news is that it’s a vaccine they made some time ago as a possible vaccine for MERS and they’ve already tested it for safety–last year actually. Safety testing can be one of the longest steps in the process of making a good vaccine. You have to watch people for quite a while to make sure they don’t have any lingering adverse effects–sometimes several years. Having something ready to test for efficacy is a big head-start. The vaccine has recently been tested in rhesus macaque monkeys with good results. Six monkeys were given the vaccine and then exposed to a large amount of the virus. All six are still healthy a month out. Testing in monkeys doesn’t guarantee success in humans but the rhesus macaque is just about the closest thing we have to humans. Given that, testing in humans is likely to happen sooner rather than later. If all goes well (that’s a gigantic IF), and the Institute is given emergency approval, they could have several million doses available as early as September. That would be monumental. Please remember there are still massive efficacy hurdles to jump so take a deep breath and in a very unscientific way, maybe cross your fingers.
With this pandemic, the rush to find an effective treatment has been fully understandable. I posted early about the possibility that hydroxychloroquine might be an effective treatment based on some very small, and it turns out pretty flawed, studies. Newer (also small, also not peer reviewed) studies out of Brazil and the VA system in the US indicate that hydroxychloroquine is ineffective in the treatment of COVID-19 and possibly dangerous (the trial in Brazil was stopped when some of the patients in the high-dose arm of the study developed lethal cardiac arrhythmias). The efficacy and safety of hydroxychloroquine to treat COVID-19 should be established in large, controlled studies and it should not be provided as an off-label treatment for the virus in a non-study setting. There, I said it. Good science takes time and patience. But nobody’s listening to me.
Look to hear from California’s Governor Newsom sometime in the next 48 hours regarding details about relaxation of the stay-at-home/social distancing orders. California’s actions have made a difference. As we’ve known for a century at least, social distancing works and it worked here. While the initial orders were emergent and broad-sweeping, look for the relaxation orders to be more surgical and to come with a period of evaluation. We needed quick, blanket action to prevent massive spread of the virus through the entire population of California when it was doubling every two days. With a doubling time of two days, the virus would have hit everyone in America within about 40 days. Now that we’re much more under control we can relax elements of social distancing one at a time with a period of observation to look for spikes. We can then see which of these measures were the most important in preventing spread of this virus. This process will give us valuable data and will help us in the fall when it’s likely the virus will surge again. Our break from the lockdown may not be as soon as we’d hoped though. This past weekend, some Californians jumped the gun and flocked to the beaches in numbers that are simply unwise at this point. This was a mistake and may very well lead to an uptick in the virus within the next two weeks. It’s just simple virology. If that happens we may not get our relaxation phase as soon as we would have, had people maintained social distancing per state and local public health department orders. Here’s hoping we don’t see that or that what we see isn’t enough to derail our break from the lockdown.



:format(webp):no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19885359/1208432585.jpg.jpg)





{kind=link}