- It’s been a time of great unrest in the Unites States and around the world after the death of George Floyd in Minneapolis at the hands of several police officers there. Demonstrations continue to occur around the country. Unquestionably we’ll see some disease surges in cities where protests occurred. Some factors that could lead to a greater surge include the use of tear gas and pepper spray which induce violent coughing, a significant driver of disease spread. Additionally, pepper spray and tear gas cause respiratory epithelial damage which could make protesters more susceptible. We know from sporting events like the UEFA Champion’s League match in Milan on February 19 between between Atalanta and Valencia that the gathering of thousands of screaming people can lead to devastating super-spreading events. Two days after that match Italy had its first case and epidemiologists feel that the match likely played a part in the region’s massive outbreak. Similarly, the protests saw much yelling likely introducing more virus into the air and onto surfaces. A mitigating factor of course, is that almost all protests occurred outdoors where dissipation of virus containing droplets occurs much faster than the still air inside buildings. We’ll likely start to see increasing cases in the next week as spikes generally occur 2-3 weeks after spreading events. Admittedly though, since there’s already a significant increase occurring in many localities due to reopening measures it may be hard to tease out causative factors.
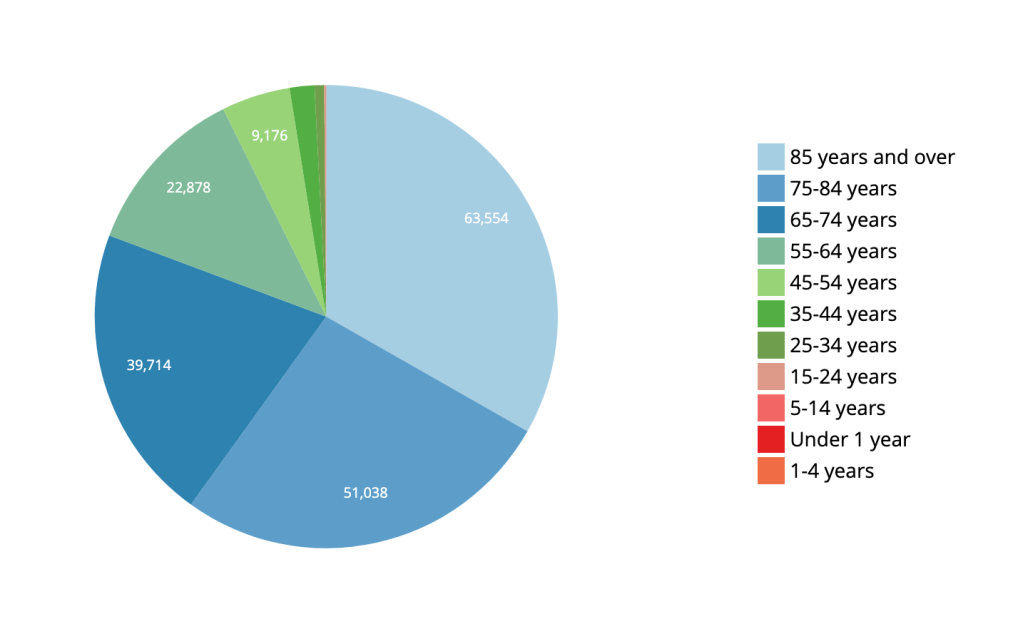
- There’s a bit of a notion that COVID-19 is merely a disease of the very old. While this disease unquestionably hits older ages disproportionately, the death toll for people pre-retirement age and younger is not insignificant. In the US, 19% of all deaths have occurred in ages 64 and below for a total of 36,906 deaths at the time of this writing. COVID-19’s disease burden is not limited to retirees and the risk to older, pre-retirement workers is substantial. This has impacts beyond death rates. The disease often leads to a long period of illness and potentially long hospitalizations. Having a significant number of employed individuals hospitalized and/or sick for extended periods of time has a measurable effect on the economy. Dismissing this disease as merely a disease of the very old is not just statistically wrong, it’s unwise on many levels for the wellbeing of the nation.
- A MMRW Early Release publication looked at how the US Air Force managed over 10,000 trainees and limited total COVID-19 cases to 5 with only 3 transmissions. Their success is no surprise to public health experts as it followed well established non-pharmaceutical interventions. Trainees were kept healthy utilizing arrival quarantine, social distancing, mandatory face coverings and rapid identification of exposed/infected individuals through rapid testing and contact tracing. As the disease grew around the country, recruits from heavily infected areas were not permitted onto the base for training. The success there indicates clearly that well-established public health interventions like those described above can very successfully prevent viral spread and can allow for business almost as usual. Just because it can’t be said too much–wear a face covering!!
- The FDA rescinded its Emergency Use Authorization for hydroxychloroquine today after reviewing the growing data demonstrating that the medication is ineffective in the treatment of COVID-19 and carries significant cardiac risk. There are still a few large trials underway examining the medication’s usefulness and safety but the FDA’s action means the medication now should not be used outside of those trials.
- There are over 135 vaccines in development for COVID-19. The most advanced trial (Phase III) is the Oxford University vaccine which is a viral vector vaccine–the spike protein from SARS-CoV-2 is delivered with a safe virus in order to generate an immune response. In the case of the Oxford vaccine that virus is an adenovirus which causes the common cold. Early data indicates that the Oxford vaccine may not prevent SARS-CoV-2 infection but it may prevent fatal illness. Even that would make the vaccine a significant step forward against COVID-19. Right on Oxford’s heels is the Moderna vaccine which is a genetic vaccine (the mechanism was discussed in an earlier post). Moderna expects to have a large scale Phase III trial underway in July. If these vaccines make it through their trials and demonstrate efficacy and safety, it’s possible that emergency use for front-line healthcare workers, first responders and highest risk individuals may be possible in late 2020. So much has to line up for that to be a reality I hesitate to mention it for fear of raising hopes too much. But it’s always nice to end on an optimistic note so here’s to hope!
