COVID-19 death counts and accusations that they have been inflated is a topic I’ve avoided writing about because it’s politically charged. When something becomes political these days it moves away from the realm of science and into the realm of dogma, or quasi-religion. That’s why I shun politics. How do you rationally and logically discuss something that contradicts an almost religiously-held political belief? It’s like trying to convince someone that your religion is far superior to theirs and that all their theological ideas and canon are wrong. No good can come from it. This is the state of politics in America. In spite of this and against my better judgement I’m going to tackle the highly politicized issue of death counts because it’s that important.
Much of this started when Dr. Scott Jensen, who also happens to be a Republican State Senator in Minnesota, claimed on Fox News that doctors were being encouraged by CDC death certificate guidelines to list COVID-19 as a diagnosis even when there’s no clear evidence of COVID-19 infection. He went on to suggest that there was a financial motivation to list COVID-19 as a diagnosis because Medicare pays $13,000 for a COVID-19 and $39,000 if that same patient is placed on a ventilator. He also stated that doctors have a different approach when caring for patients with influenza. He used a hypothetical case of a patient with influenza who died during the course of the illness with a pneumonia as well. For him that death would be due to respiratory failure and pneumonia.
Jensen gave a hypothetical example of a patient who died while suffering from influenza. If the patient was elderly and had symptoms like fever and cough a few days before passing away, the doctor explained, he would have listed “respiratory arrest” as the primary cause of death.
“I’ve never been encouraged to [notate ‘influenza’],” he said. “I would probably write ‘respiratory arrest’ to be the top line, and the underlying cause of this disease would be pneumonia … I might well put emphysema or congestive heart failure, but I would never put influenza down as the underlying cause of death and yet that’s what we are being asked to do here.”
Dr. Scott Jensen/Fox News
Dr. Jensen and others have also called into question a CARES Act provision that pays hospitals a 20% bump over Medicare payments for patients with COVID-19. With financial incentives like this the clear implication is that doctors and hospitals are cooking the books, in effect, to unethically profit off of the crisis. There also seems to be a growing sentiment that above and beyond financial interests, that COVID-19 deaths are inflated in order to damage the President and increase the likelihood that he will lose the general election in November.
There’s a lot to unpack here but I’ll do my best. As always, I’m going to do my best to steer clear of politics and just try to address the accusations. For me, the most important reason to answer the allegations because of the damage they unfairly do to the public’s trust of doctors, hospitals and public health system. I’ll briefly discuss Dr. Jensen’s claims and why they don’t make sense to me. Ultimately you may choose to believe him over me but know that I don’t have a financial interest in COVID-19. On the contrary, as long as this crisis disrupts the economy my family is taking a financial hit like so many other American households. Life will unquestionably be better for me when this is over; I have no desire to make it seem worse than it is or drag it out longer than needed. I do have a great desire to help people understand how truly dangerous this virus is which is a different thing altogether. After I address Dr. Jensen, I will provide some data that I think shows pretty clearly that numbers aren’t exaggerated, in all likelihood COVID-19 deaths are undercounted.
Let’s take a look at the claim that hospitals get $13,000 for a COVID-19 admission and $39,000 for ventilation of a patient with the same diagnosis. These numbers are pretty close to the truth but what Dr. Jensen didn’t mention is that they are taken from the same diagnosis-related group (DRG) that covers other similar respiratory conditions. The Kaiser Family Foundation found that “average Medicare payment for respiratory infections and inflammations with major comorbidities or complications in 2017, which was $13,297.” They also found that “the average Medicare payment for a respiratory system diagnosis with ventilator support for greater than 96 hours…was $40,218.” So the base payment for hospitalization and/or ventilation for COVID-19 is actually pretty much identical to the payment for similar respiratory conditions. Well, what about the 20% bump you might ask? It is definitely true that this bump exists; it is part of the CARES Act that Congress passed and the President signed to help get the country through the crisis. The 20% bump is designed to help hospitals cover the added costs of caring for COVID-19 patients including personal protective equipment, isolation and disinfecting costs, and in particular the cost of caring for the uninsured. By paying a bit more for every Medicare patient, hospitals are better able to handle the added costs of caring for patients who have no insurance and likely will never be able to fully pay for their care assuming they survive to try.
As far as Dr. Jensen’s accusation of pressure to list COVID-19 on death certificates I’d also argue that the CDC’s guidance on certifying COVID-19 deaths is not unreasonable. This is based on my experience as a physician and public health doctor during the crisis. I definitely don’t think that this is resulting in a statistically significant over-counting of COVID-19 but more on that later in the post. Here’s the CDC’s exact wording.
In cases where a definite diagnosis of COVID-19 cannot be made, but it is suspected or likely (e.g., the circumstances are compelling within a reasonable degree of certainty), it is acceptable to report COVID–19 on a death certificate as “probable” or “presumed.” in these instances, certifiers should use their best clinical judgement in determining if a COVID–19 infection was likely. However, please note that testing for COVID–19 should be conducted whenever possible.
Guidance for Certifying Deaths Due to Coronavirus Disease 2019 (COVID–19)
You don’t have to believe me on this but this practice is not unusual for certification of death. There has never been a cookbook method of listing causes of death. For patients with infectious diseases, high suspicion based on clinical presentation and exposure history can inform decisions about cause of death even in the absence of laboratory tests. I fully disagree with Dr. Jensen on one of his points. He suggested in his Fox News interview that he never codes a patient who has tested positive for influenza as an influenza death if the patient has pneumonia. He reports he would list that death as respiratory failure and pneumonia. I do not believe that is the practice of the majority of US physicians nor do I believe it is appropriate. For patients such as this, the acute illness with influenza, should at least be included as a secondary diagnosis as it certainly contributed to the patient’s death.
So enough about Dr. Jensen. Let’s take a look at the data that to me shows that deaths are indeed real and not over-counted. The data shows they are actually significantly undercounted. The New York Times has been tracking year to year differences in deaths in seven states with some interesting results. When compared to the previous five years New York City for instance had 225% more deaths (11,900) this year between March 8 and April 11 than the same period for the last five years–no year came anywhere close. The rest of New York had 42% (4200) more deaths than previous years and New Jersey had 72% (5200) more. Other states showed the same trend: Michigan had 21% (2000), Illinois came in at 13% (1400) and Massachusetts was higher by 20% (1200). Where did these deaths come from if not COVID-19? Did we suddenly have large aberrant spike in trauma deaths or cardiac deaths or cancer deaths in multiple states this spring? I think it would test the bounds of credulity to suggest this is the case. The truth is, I think, simpler; this spring we were hit with a dangerous virus that can hide in seemingly healthy people and spread easily to close contacts causing a disturbingly common severe respiratory distress syndrome with or without multisystem organ failure.
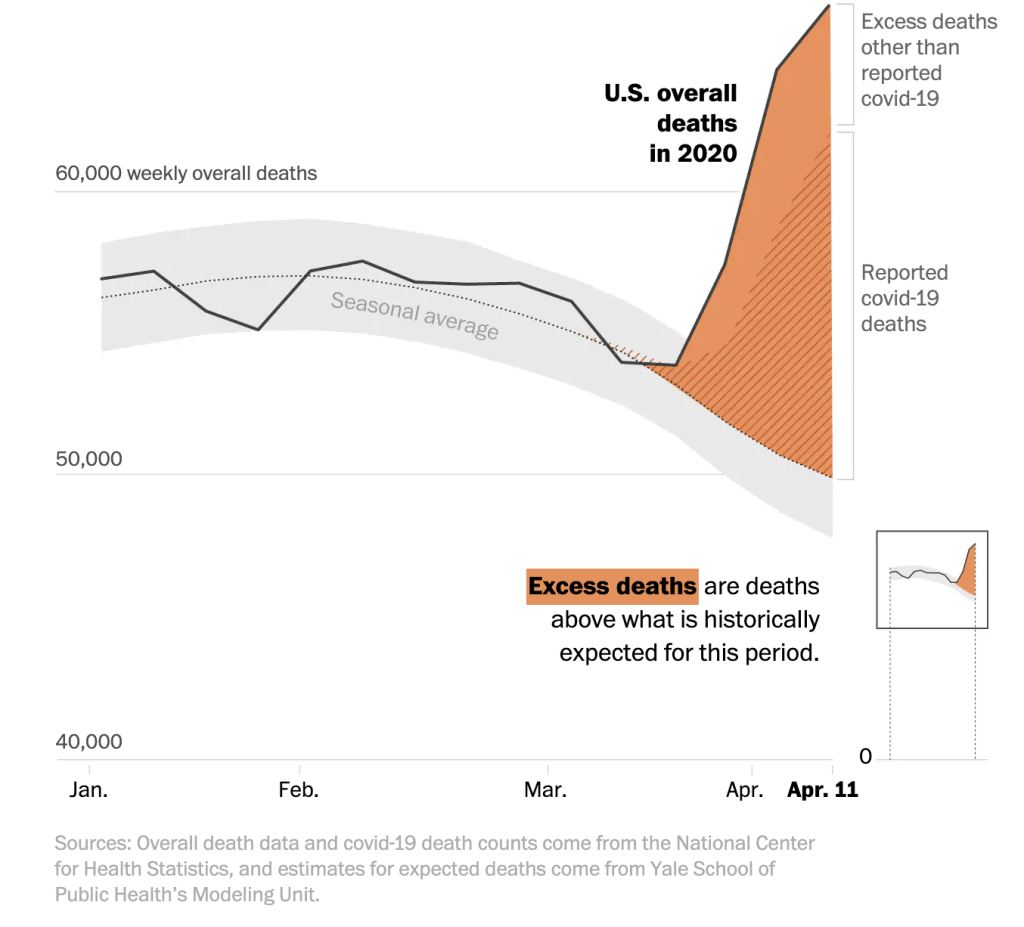
If that’s not enough, consider this. In all of the states I mentioned and that the Times followed, the number of confirmed COVID-19 deaths is lower than the total number of extra deaths. In other words, COVID-19 deaths were undercounted in NYC (1700), NJ (3000), NY State (1700), Michigan (600), Illinois (700) and Massachusetts (500) over that time period. The Washington Post looked at the early days of the pandemic and measured excess deaths across the country and found similar data–we had far more deaths than normal years and there’s solid evidence that we didn’t catch all of the COVID-19 cases.
I can understand that some Americans may have doubts about COVID-19 numbers, particularly when physicians step forward to suggest that something fishy is going on. It’s reasonable to feel this way and it’s important to hear out critics of any system. I don’t believe Dr. Jensen is lying and I don’t believe he is a bad person. He’s undoubtedly an excellent, dedicated doctor to the patients in his practice. I think just think he’s wrong about this and in my mind the data confirms this.
